At Evoca, you will meet your GP and discuss your medical history to make sure its the right solution for you.
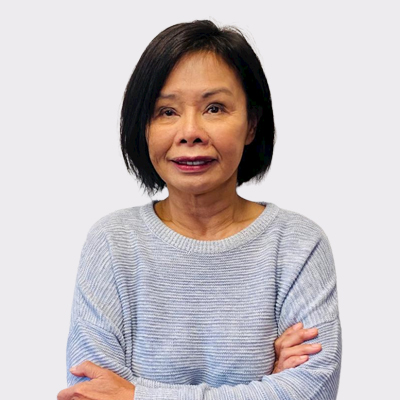
Mirena IUD is a hormone releasing intrauterine device . It is a small T shaped plastic device with a central chamber containing a progesterone hormone called levornogestrel, which is released slowly via a controlled mechanism over 5 years into the uterine cavity. It is indicated for contraceptive purposes, and for the management of heavy menstrual bleeding. It can also be used for endometrial protection in the context of estrogen replacement in the menopause.
in its contraceptive effect, it thickens the mucous in the cervical canal, making it more difficult for the sperm to swim into the uterus and affects the ability of the egg and sperm to move through the fallopian tubes, which reduces the chances of fertilisation of the egg. Additionally the effect of exposing the endometrium to continuous low dose levornogestrel causes thinning of the endometrium, making it less suitable for implantation and pregnancy. This thinning of the endometrium means that while ovulation continues unchanged, blood loss associated with periods is usually significantly reduced, and in many cases women may stop menstruating altogether owing to the lack of endometrial tissue to shed at the usual time of menstruation. Up to 70% of women have no or minimal menstrual flow after Mirena insertion, and those who continue to menstruate experience up to 93% reduction in menstrual flow.

Most Mirena insertions are uncomplicated, however to discuss your individual risks we recommend you speak to your Evoca doctor to ensure you understand the risks associated with your particular case, and how your doctor can help you mitigate these.
Come prepared with a history of your contraceptive use, and details around why they weren’t suitable.
Be ready to describe your cycle and tell us when your last period was.
If you have any family history of illnesses, let us know. This may affect the contraceptive choice so knowing your family history will help us tailor your contraception better.
If you are considering an IUD or implant, you will be provided with instructions on how best to prepare for the day of your fitting. Your GP will discuss with you when your fitting can take place as it needs to be fitted at the right time of your cycle to optimise contraceptive cover.

General Practitioner

General Practitioner

General Practitioner

General Practitioner

General Practitioner

General Practitioner

General Practitioner
General Practitioner

General Practitioner

General Practitioner

General Practitioner

Specialist Obstetrician and Gynaecologist

General Practitioner

General Practitioner

General Practitioner

General Practitioner
General Practitioner
General Practitioner
General Practitioner

General Practitioner

General Practitioner
The fitting procedure only takes a few minutes, and you will be able to go home straight afterward. Your GP will routinely review you a month after the fitting to ensure all is going well and that you aren’t having any problems post insertion.
No, studies have consistently failed to demonstrate conclusively that the contraceptive implant causes weight gain.
The hormonal IUDs release a small amount of progesterone which thins the lining of the womb. This can make periods lighter, or sometimes even disappear, despite ongoing ovulation.
The copper IUD generally doesn’t change the cycle but can, in a small proportion of women, cause increased bleeding.
No, your partner should not feel the threads. Sometimes the threads may be a little long post insertion and we can trim these at your check-up visit, 1 month after insertion.
Inserting of the IUD involves a brief period of discomfort during the procedure, but after this and once the device has settled, you should not experience ongoing pain or discomfort.
No, IUDs can be inserted in any woman who is sexually active and does not have an abnormality of her vagina, cervix or uterus. The Kyleena is a specially developed smaller sized IUD designed to fit in women who have not given birth.
No, but the combined pill (with estrogen and progesterone) stops ovulation, so with prolonged use, it can take time after stopping for ovulation to return – this can be up to 12 months.